





Cataract Surgery
Intraocular lenses
The intraocular lens is made from a type of plastic that is moulded or cut provide a lens of a particular strength. Every eye is unique and the strength of the IOL that is required will vary from patient to patient. A range of strengths is available to allow the most suitable lens to be selected for each eye.
There are numerous manufacturers that provide IOLs and most will also have a selection of lens types. The type of lens that is best suited to your eye will depend on your biometry (a list of eye measurements made prior to surgery) as well as personal preference and I we will explore these lens types below.
An IOL is selected primarily to provide clear distance vision. All the IOLs will achieve this.
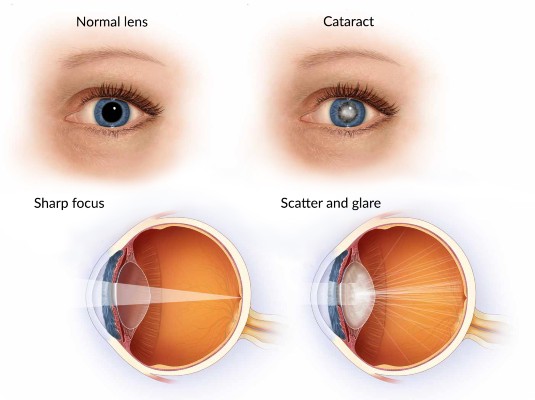
An IOL that provides only distance vision is referred to as monofocal, meaning that it only focuses on one place (distance), which for practical purposes means everything further than about 2 or 3 meters away. Anything closer that this will become increasingly blurred.
In addition, some IOLs will provide intermediate or near vision as well, and these may be referred to as multifocal IOLs.
There is also an option to correct astigmatism with an intraocular lens known as a toric lens.
A normal cornea has a uniform curvature, like a soccer ball.
A cornea with astigmatism is more curved in one direction than the other, like a rugby ball.
A cornea with astigmatism is unable to focus light sharply unless the light passes through a second lens that can correct the astigmatism. This is effectively what the optometrist does when prescribing glasses. The correcting lens can also be the toric intraocular lens that is placed at the time of surgery. The advantage of this approach is that good vision is now possible without glasses.
Broadly speaking the monofocal IOL will have the lowest risk of visual disturbance after cataract surgery.
Multifocal IOLs have concentric grooves on the surface which allows the lens to focus over a larger range. However, this design introduces the possibility of visual disturbance in the form of glare and halos. The halos are visible when looking at lights at night and vary from barely noticeable to significant.
It appears that a greater the degree of near vision correction correlates to a greater risk of visual disturbance.
 Cataract surgery is one of the most frequently performed operations worldwide and 99.5% of patients have no complications. However, there is always a small risk with any procedure, and this will be discussed with you in detail before you decide to proceed with surgery.
Cataract surgery is one of the most frequently performed operations worldwide and 99.5% of patients have no complications. However, there is always a small risk with any procedure, and this will be discussed with you in detail before you decide to proceed with surgery.
Image: IOL Range
Cataract surgery is one of the most frequently performed operations worldwide and 99.5% of patients have no complications. However, there is always a small risk with any procedure, and this will be discussed with you in detail before you decide to proceed with surgery.